Introduction
Shortness of breath is one of the most common reasons people seek medical attention, yet the underlying cause is not always immediately obvious. Two chronic conditions that frequently produce breathing difficulties are congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD). Although these disorders affect different organs and arise from different disease processes, they often share similar symptoms, making diagnosis challenging.
Both congestive heart failure and COPD affect millions of people worldwide and are major causes of disability, hospitalization, and reduced quality of life. Patients living with either condition may experience fatigue, exercise intolerance, persistent coughing, and difficulty performing everyday activities. In some cases, an individual may even have both conditions simultaneously, which can further complicate diagnosis and treatment.
Understanding the differences between congestive heart failure and COPD is essential for patients, caregivers, and healthcare professionals. Accurate diagnosis allows for appropriate treatment, improved symptom control, and better long-term outcomes. This article explores how these conditions differ, where they overlap, and what treatment strategies are available to help individuals manage their symptoms effectively.
Understanding Congestive Heart Failure
Congestive heart failure is a chronic condition in which the heart becomes unable to pump blood efficiently enough to meet the body’s needs. Contrary to what the name suggests, heart failure does not mean that the heart has stopped working entirely. Rather, it indicates that the heart’s pumping ability has been weakened or impaired.
When the heart cannot circulate blood effectively, blood may begin to back up into various parts of the body. This backup of blood increases pressure within the blood vessels and often leads to fluid accumulation in the lungs, abdomen, legs, and other tissues. The resulting congestion is responsible for many of the symptoms associated with heart failure.
Heart failure can affect either the left side, the right side, or both sides of the heart. Left-sided heart failure is the most common form and frequently causes fluid accumulation in the lungs, leading to breathing difficulties. Right-sided heart failure often causes swelling in the legs, ankles, feet, and abdomen due to fluid retention in peripheral tissues.
Related Posts:




Healthcare providers also classify heart failure according to how well the heart contracts. In systolic heart failure, also known as heart failure with reduced ejection fraction (HFrEF), the heart muscle cannot contract effectively. In diastolic heart failure, also called heart failure with preserved ejection fraction (HFpEF), the heart becomes stiff and cannot fill properly between beats.
Several underlying conditions can lead to congestive heart failure. Coronary artery disease remains one of the most common causes because reduced blood flow can weaken the heart muscle over time. Other important contributors include high blood pressure, diabetes, heart valve disorders, cardiomyopathy, and previous heart attacks.
Understanding COPD
Chronic obstructive pulmonary disease is a progressive lung disorder characterized by persistent airflow limitation. Unlike congestive heart failure, which primarily affects the cardiovascular system, COPD directly damages the lungs and airways, making it increasingly difficult for air to move in and out of the respiratory system.
COPD is not a single disease but rather a term used to describe a group of chronic lung conditions. The two most common forms are chronic bronchitis and emphysema.
Chronic bronchitis involves long-term inflammation of the bronchial tubes, the airways that carry air to and from the lungs. This inflammation causes excessive mucus production, leading to chronic coughing and airway obstruction.
Emphysema involves destruction of the tiny air sacs known as alveoli. These structures are responsible for oxygen exchange between the lungs and bloodstream. As alveoli become damaged, less oxygen enters the blood, and breathing becomes increasingly difficult.
Smoking is by far the leading cause of COPD. Long-term exposure to tobacco smoke damages lung tissue and triggers chronic inflammation. However, COPD can also result from exposure to environmental pollutants, occupational dusts, chemical fumes, biomass fuel smoke, and certain genetic conditions such as alpha-1 antitrypsin deficiency.
Because COPD is progressive, symptoms typically worsen over time if the disease is not properly managed.
Similar Symptoms Between CHF and COPD
One reason CHF and COPD are frequently confused is that both conditions produce similar symptoms. In both disorders, the body’s ability to deliver oxygen efficiently becomes compromised, resulting in many overlapping clinical manifestations.
Shortness of breath is perhaps the most recognizable symptom shared by both conditions. Individuals with either CHF or COPD often experience difficulty breathing during physical activity, and symptoms may gradually worsen as the disease progresses.
Fatigue is another common complaint. Reduced oxygen delivery to tissues can leave patients feeling weak, exhausted, and unable to maintain their usual activity levels.
Exercise intolerance is also frequently present. Activities that once seemed routine, such as climbing stairs, carrying groceries, or walking moderate distances, may become increasingly challenging.
Both conditions can produce coughing. However, the nature of the cough often differs and can provide important diagnostic clues.
Sleep disturbances are common as well. Breathing difficulties may interrupt sleep and contribute to poor daytime energy levels.
Despite these similarities, important differences exist that help distinguish one condition from the other.
Key Differences Between Congestive Heart Failure and COPD
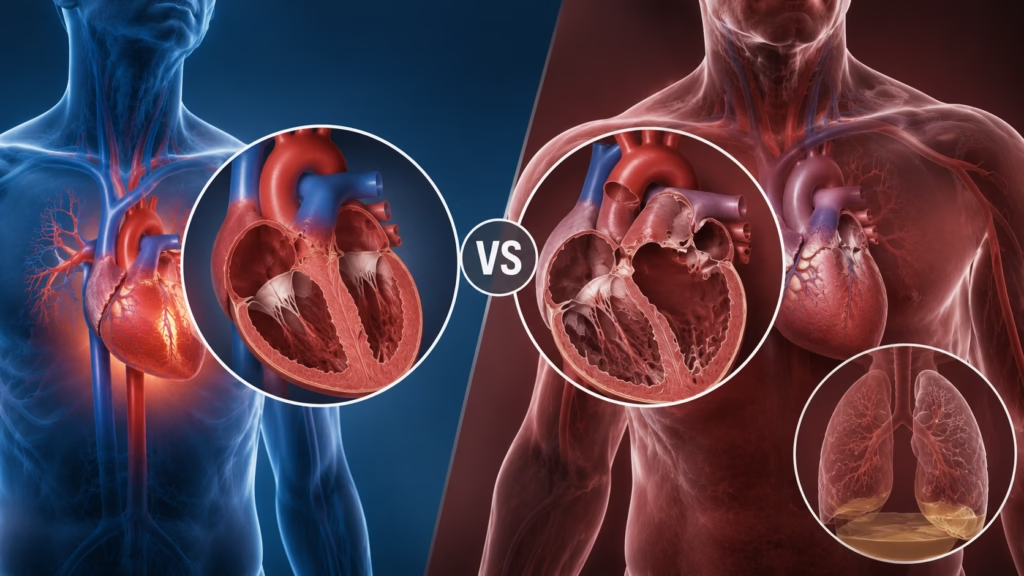
Although both conditions cause breathlessness, the underlying mechanisms are very different.
Congestive heart failure originates in the cardiovascular system. The primary problem is the heart’s inability to pump blood effectively. As blood backs up into the lungs and other tissues, fluid accumulation develops, causing congestion and breathing difficulties.
COPD originates in the respiratory system. The primary problem is obstruction of airflow caused by damaged airways and lung tissue. Oxygen exchange becomes less efficient because of inflammation, mucus production, and destruction of alveolar structures.
The pattern of symptoms often differs between the two conditions. Individuals with heart failure frequently notice worsening breathlessness when lying flat. This symptom, known as orthopnea, occurs because fluid shifts toward the lungs when a person reclines. Many patients find relief by sleeping with extra pillows or elevating the head of the bed.
People with COPD are more likely to experience persistent wheezing, chronic mucus production, and prolonged coughing. Their symptoms are often triggered by respiratory infections, environmental pollutants, or physical exertion.
Swelling of the ankles, feet, and legs is much more common in congestive heart failure due to fluid retention. While advanced COPD can sometimes cause swelling, it is generally less prominent and usually occurs later in the disease course.
The type of cough may also differ. Heart failure often produces a dry cough or a cough associated with pink, frothy sputum during severe episodes of pulmonary edema. COPD more commonly produces a productive cough containing mucus.
Causes and Triggers
The causes of CHF and COPD differ substantially because each condition affects a different organ system.
Congestive heart failure often develops after years of cardiovascular stress. Coronary artery disease, high blood pressure, heart valve abnormalities, cardiomyopathy, and previous heart attacks can all weaken the heart muscle and impair its ability to pump effectively.
Certain events can trigger sudden worsening of heart failure symptoms. These include excessive sodium intake, uncontrolled blood pressure, heart rhythm disturbances, infections, medication non-adherence, and fluid overload.
COPD is primarily linked to chronic lung damage. Long-term cigarette smoking remains the leading risk factor worldwide. Additional contributors include occupational exposure to dust and chemicals, air pollution, repeated respiratory infections, and inherited genetic disorders.
COPD exacerbations are commonly triggered by viral infections, bacterial infections, poor air quality, and exposure to smoke or other respiratory irritants.
How Doctors Diagnose CHF and COPD
Accurate diagnosis is critical because treatments differ significantly between the two conditions.
When congestive heart failure is suspected, physicians begin with a detailed medical history and physical examination. Signs such as leg swelling, elevated neck veins, and abnormal heart sounds may point toward heart failure.
An echocardiogram is one of the most important diagnostic tests because it provides detailed information about heart structure and function. It allows healthcare providers to measure ejection fraction and identify valve abnormalities.
Blood tests measuring B-type natriuretic peptide (BNP) or NT-proBNP are often used because elevated levels suggest increased cardiac stress and heart failure.
Chest imaging may reveal fluid accumulation in the lungs or enlargement of the heart.
For COPD, spirometry is the cornerstone of diagnosis. This pulmonary function test measures airflow and determines how effectively the lungs move air. A reduced FEV1/FVC ratio confirms airflow obstruction consistent with COPD.
Chest X-rays and CT scans may reveal hyperinflated lungs, emphysema, or other structural abnormalities. Arterial blood gas testing may be performed to evaluate oxygen and carbon dioxide levels in more advanced cases.
Treatment of Congestive Heart Failure
The treatment of heart failure focuses on improving heart function, reducing symptoms, preventing hospitalizations, and prolonging survival.
Several medication classes form the foundation of modern heart failure treatment. ACE inhibitors and angiotensin receptor blockers help reduce the workload on the heart and improve long-term outcomes. Beta-blockers slow the heart rate and reduce stress on the cardiovascular system. Diuretics help remove excess fluid from the body, reducing swelling and relieving breathlessness.
Newer therapies such as angiotensin receptor-neprilysin inhibitors and SGLT2 inhibitors have further improved outcomes for many patients.
In some cases, specialized devices such as implantable cardioverter-defibrillators or cardiac resynchronization therapy devices may be recommended. Advanced cases may require valve repair, coronary artery bypass surgery, ventricular assist devices, or heart transplantation.
Treatment of COPD
COPD treatment aims to improve airflow, reduce symptoms, prevent exacerbations, and enhance quality of life.
Bronchodilators are commonly prescribed to relax airway muscles and improve breathing. Depending on disease severity, patients may use short-acting or long-acting formulations.
Inhaled corticosteroids may be added to reduce airway inflammation in selected patients, particularly those with frequent exacerbations.
Pulmonary rehabilitation programs combine exercise training, breathing techniques, education, and nutritional counseling to improve overall function and symptom management.
Supplemental oxygen therapy may be necessary for individuals with chronically low oxygen levels. Vaccinations against influenza and pneumonia are strongly recommended because respiratory infections can cause severe COPD flare-ups.
When CHF and COPD Occur Together
It is not uncommon for patients to have both congestive heart failure and COPD simultaneously. This coexistence is particularly common among older adults and individuals with a history of smoking.
Managing both conditions requires careful coordination because symptoms often overlap and treatments must be balanced carefully. Certain medications used for one condition may affect the other, making specialist involvement especially important.
A collaborative healthcare team consisting of cardiologists, pulmonologists, primary care physicians, pharmacists, respiratory therapists, and rehabilitation specialists often provides the best outcomes.
Lifestyle Strategies for Both Conditions
Lifestyle modifications play a crucial role in managing both CHF and COPD.
Patients with heart failure should monitor sodium intake carefully, weigh themselves regularly, and follow prescribed fluid restrictions when recommended. Smoking cessation is critical for all patients but particularly essential for those with COPD.
Regular physical activity tailored to individual capabilities can improve endurance, reduce symptoms, and enhance overall quality of life. Maintaining a healthy diet rich in fruits, vegetables, whole grains, and lean proteins supports both heart and lung health.
Breathing exercises such as diaphragmatic breathing and pursed-lip breathing may help individuals with COPD manage breathlessness more effectively.
Consistent follow-up appointments, medication adherence, and prompt reporting of worsening symptoms are vital for long-term disease management.
Conclusion
Congestive heart failure and chronic obstructive pulmonary disease are two serious chronic conditions that frequently produce similar symptoms, particularly shortness of breath and fatigue. However, despite these similarities, they originate from entirely different disease processes. Heart failure results from impaired cardiac function and fluid congestion, whereas COPD stems from chronic damage to the lungs and airways.
Understanding the distinctions between these conditions is essential because accurate diagnosis directly influences treatment decisions and long-term outcomes. Modern therapies, lifestyle modifications, and comprehensive medical care have significantly improved the outlook for individuals living with either condition.
Anyone experiencing persistent breathlessness, chronic coughing, swelling, fatigue, or reduced exercise tolerance should seek medical evaluation. Early diagnosis and appropriate treatment can help control symptoms, reduce complications, and improve overall quality of life. While CHF and COPD present unique challenges, many individuals successfully manage these conditions and continue to lead active, meaningful lives with the right support and treatment plan.
Disclaimer
This article is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment. Seizures, severe headache, confusion, visual changes, or blood pressure readings in the hypertensive crisis range require urgent medical evaluation.