Introduction
Heart disease remains one of the leading causes of illness and death worldwide, and among the many cardiovascular conditions that affect millions of people, atrial fibrillation (AFib) and congestive heart failure (CHF) are two of the most common. Although they are distinct medical conditions with different underlying mechanisms, they often occur together and can significantly impact a person’s quality of life, physical functioning, and long-term health outcomes.
Many patients are understandably confused when they hear terms such as “atrial fibrillation” and “heart failure” used during medical appointments. Both conditions can cause fatigue, shortness of breath, reduced exercise tolerance, and hospitalizations. However, AFib primarily involves an abnormal heart rhythm, whereas congestive heart failure is a disorder of the heart’s pumping ability. Understanding these differences is essential because each condition requires a unique approach to diagnosis, treatment, and ongoing management.
At the same time, AFib and CHF frequently influence one another. A patient with long-standing atrial fibrillation may eventually develop heart failure due to chronic strain on the heart. Similarly, individuals with heart failure often develop atrial fibrillation because structural changes within the heart create an environment that promotes abnormal electrical activity. As a result, healthcare providers frequently manage both conditions simultaneously.
This comprehensive guide explains what atrial fibrillation and congestive heart failure are, highlights their differences and similarities, explores how they overlap, and discusses practical strategies for treatment and prevention.
What Is Atrial Fibrillation (AFib)?
Atrial fibrillation is the most common sustained cardiac arrhythmia encountered in clinical practice. It occurs when the heart’s upper chambers, known as the atria, experience chaotic electrical signals that cause them to quiver or fibrillate instead of contracting in an organized manner.
Under normal circumstances, electrical impulses originate from the sinoatrial node, often referred to as the heart’s natural pacemaker. These signals travel through the atria and then to the ventricles, producing a coordinated heartbeat. In atrial fibrillation, this orderly process becomes disrupted. Multiple electrical impulses fire simultaneously throughout the atria, causing rapid and irregular contractions.
Related Posts:




Because the atria do not contract effectively, blood may pool within these chambers rather than moving efficiently into the ventricles. This pooling increases the risk of blood clot formation. If a clot travels from the heart to the brain, it can block blood flow and cause a stroke.
The symptoms of atrial fibrillation vary widely among individuals. Some patients experience noticeable palpitations, which may feel like fluttering, racing, pounding, or irregular heartbeats. Others may report fatigue, dizziness, weakness, chest discomfort, or shortness of breath. Interestingly, some individuals have no symptoms at all and discover their condition only during routine medical examinations.
Several factors increase the likelihood of developing AFib. Advanced age is one of the strongest risk factors. Other contributors include high blood pressure, coronary artery disease, obesity, diabetes, sleep apnea, excessive alcohol consumption, thyroid disorders, and structural abnormalities of the heart.
What Is Congestive Heart Failure (CHF)?
Congestive heart failure is a chronic clinical syndrome that occurs when the heart cannot pump enough blood to meet the body’s metabolic demands. Contrary to what the name suggests, heart failure does not mean that the heart has stopped working entirely. Rather, it means that the heart’s pumping efficiency has been reduced.
The heart functions as a powerful pump responsible for delivering oxygen-rich blood to organs and tissues throughout the body. When this pumping ability becomes impaired, blood circulation slows, and fluid may accumulate in various parts of the body. This fluid buildup is responsible for many of the symptoms associated with congestive heart failure.
Heart failure is generally classified into two broad categories. Systolic heart failure occurs when the heart muscle becomes weakened and cannot contract forcefully enough to eject blood efficiently. Diastolic heart failure occurs when the heart muscle becomes stiff and cannot relax properly between beats, limiting its ability to fill with blood.
Numerous conditions can lead to congestive heart failure. Coronary artery disease is one of the most common causes because it reduces blood supply to the heart muscle. Long-standing hypertension forces the heart to work harder and may eventually weaken its function. Heart valve disease, cardiomyopathy, congenital heart defects, and previous heart attacks can also contribute to the development of CHF.
Common symptoms include shortness of breath, fatigue, swelling of the legs and ankles, rapid weight gain from fluid retention, persistent coughing, and difficulty lying flat due to breathing problems. As the condition progresses, patients may find it increasingly difficult to perform routine activities.
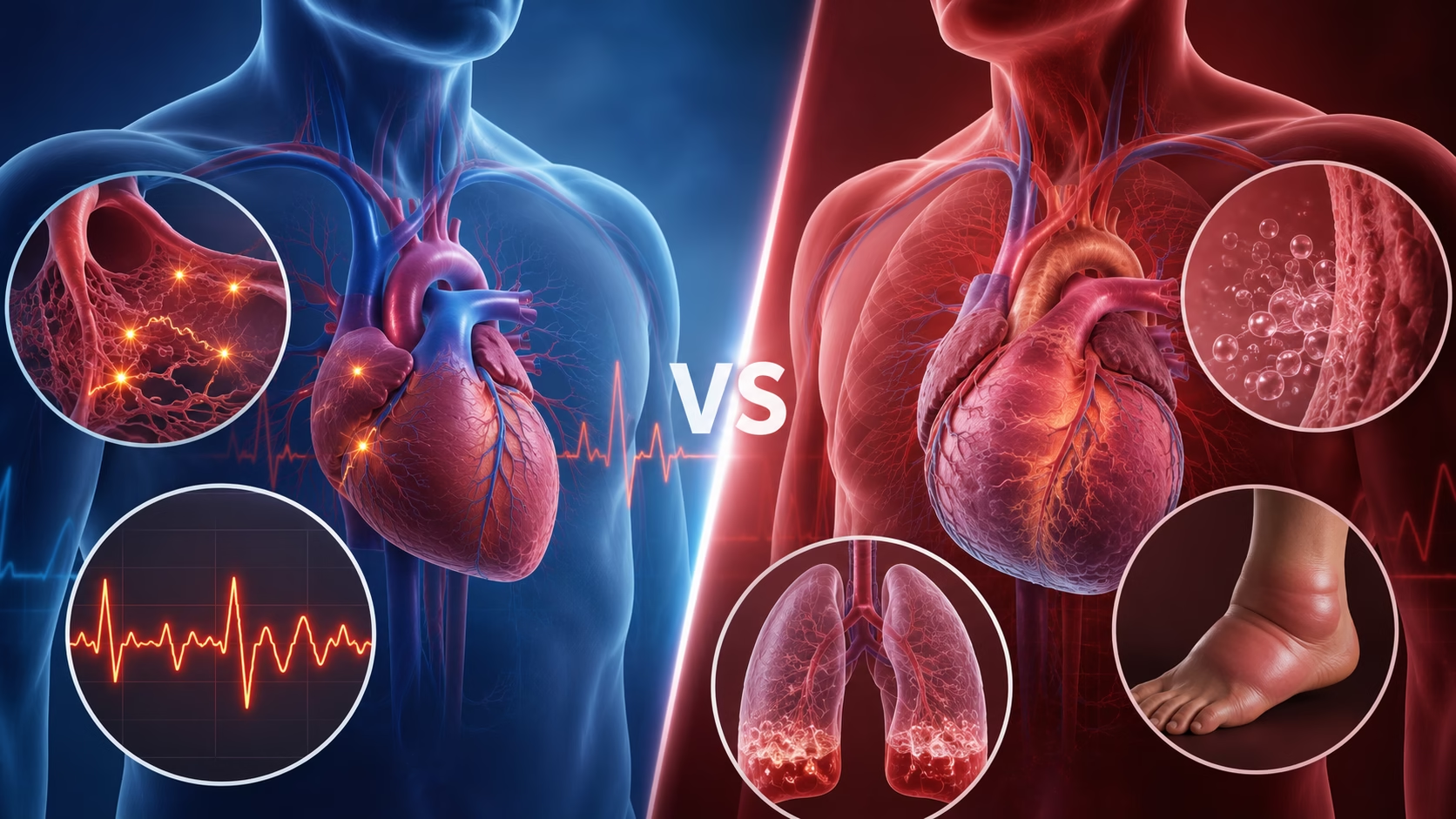
The Fundamental Difference Between AFib and CHF
Although AFib and CHF both affect cardiovascular function, their underlying mechanisms are very different.
Atrial fibrillation is primarily an electrical disorder. The problem originates in the heart’s electrical system, causing irregular and often rapid heartbeats. The heart muscle itself may initially remain structurally normal.
Congestive heart failure, on the other hand, is primarily a mechanical disorder. The heart’s pumping function becomes impaired due to weakened muscle, stiff chambers, or structural abnormalities. While electrical disturbances may occur in CHF, they are not the primary cause of the syndrome.
Another major distinction involves the primary risks associated with each condition. In AFib, the greatest concern is often stroke caused by blood clots that form within the atria. In CHF, the primary concern is progressive fluid accumulation, organ congestion, and inadequate circulation to vital tissues.
These differences influence treatment decisions and long-term management strategies.
Shared Symptoms and Clinical Overlap
Despite their distinct causes, AFib and CHF frequently produce similar symptoms, which can sometimes make diagnosis challenging.
Shortness of breath is one of the most common symptoms shared by both conditions. In AFib, breathing difficulties may occur because the irregular heartbeat reduces cardiac efficiency. In CHF, fluid accumulation in the lungs interferes with oxygen exchange and contributes to breathlessness.
Fatigue is another symptom commonly reported by patients with either condition. Reduced blood flow and inefficient circulation can limit oxygen delivery to muscles and organs, leading to decreased energy levels.
Exercise intolerance is also common. Patients may find that activities they once performed easily now leave them exhausted or breathless.
Swelling in the legs, ankles, and abdomen may occur in both conditions, although it is generally more characteristic of congestive heart failure.
Because symptoms overlap significantly, healthcare providers often rely on diagnostic testing to determine whether AFib, CHF, or both conditions are present.
How AFib and CHF Influence Each Other
The relationship between atrial fibrillation and congestive heart failure is complex and bidirectional.
In some patients, uncontrolled atrial fibrillation leads to heart failure. When the heart beats too rapidly for prolonged periods, the ventricles may become weakened and enlarged. This condition, known as tachycardia-induced cardiomyopathy, can eventually reduce the heart’s pumping efficiency and result in CHF.
Conversely, heart failure creates structural and electrical changes within the heart that increase the risk of AFib. Elevated pressures within the heart chambers cause stretching of the atria, which disrupts normal electrical pathways and promotes arrhythmias.
Once both conditions coexist, each tends to worsen the other. Atrial fibrillation reduces cardiac efficiency and may exacerbate heart failure symptoms, while heart failure increases the likelihood of recurrent AFib episodes.
This creates a cycle that often requires aggressive and coordinated treatment.
Diagnostic Evaluation
Accurate diagnosis is essential because treatment strategies differ significantly between AFib and CHF.
Diagnosing Atrial Fibrillation
The cornerstone of AFib diagnosis is the electrocardiogram (ECG). An ECG records the heart’s electrical activity and can reveal the characteristic irregular rhythm associated with atrial fibrillation.
For patients whose symptoms occur intermittently, physicians may recommend Holter monitoring or event recorders that continuously monitor heart rhythm over extended periods.
An echocardiogram is often performed to assess heart structure, evaluate chamber size, and identify any underlying abnormalities that may contribute to AFib.
Diagnosing Congestive Heart Failure
Diagnosis of CHF begins with a detailed medical history and physical examination. Healthcare providers look for signs of fluid retention, abnormal heart sounds, lung congestion, and swelling.
Echocardiography is the most important imaging test for heart failure because it provides information about ejection fraction, chamber size, wall motion, and valve function.
Blood tests measuring BNP or NT-proBNP levels help identify increased cardiac stress and support the diagnosis of heart failure.
Chest X-rays may reveal heart enlargement and fluid accumulation in the lungs.
Treatment Strategies for Atrial Fibrillation
The management of AFib focuses on three primary goals: controlling heart rate, restoring or maintaining normal rhythm when appropriate, and preventing stroke.
Medications such as beta-blockers and calcium channel blockers are commonly used to control heart rate. These medications help slow the heart and improve its efficiency.
Rhythm-control medications may be prescribed to restore normal heart rhythm or reduce the frequency of AFib episodes. Examples include amiodarone and other antiarrhythmic drugs.
Stroke prevention is a critical component of AFib management. Blood thinners such as warfarin or direct oral anticoagulants help reduce the risk of clot formation and stroke.
For some patients, catheter ablation offers a more definitive treatment option. During this procedure, abnormal electrical pathways within the heart are identified and destroyed using specialized energy sources.
Treatment Strategies for Congestive Heart Failure
The treatment of CHF focuses on improving cardiac function, reducing symptoms, preventing disease progression, and minimizing hospitalizations.
Diuretics are frequently used to remove excess fluid and reduce swelling. These medications help alleviate shortness of breath and improve comfort.
ACE inhibitors, angiotensin receptor blockers, and newer heart failure medications help reduce the workload on the heart and improve long-term outcomes.
Beta-blockers slow the heart rate and reduce stress on the heart muscle, improving survival in many patients with heart failure.
For selected individuals, implanted devices such as implantable cardioverter-defibrillators (ICDs) or cardiac resynchronization therapy (CRT) devices can significantly improve outcomes.
Managing Patients with Both AFib and CHF
Patients with both conditions require careful coordination of care. Treatment decisions must balance the goals of controlling heart rhythm, improving cardiac function, reducing symptoms, and preventing complications.
Healthcare providers often use combinations of medications to optimize heart rate, reduce fluid retention, and prevent stroke. Frequent follow-up appointments and monitoring are necessary to adjust treatment plans as conditions evolve.
Many patients benefit from collaborative care involving cardiologists, electrophysiologists, primary care physicians, pharmacists, and specialized heart failure teams.
Lifestyle Changes That Support Heart Health
Lifestyle modifications are fundamental to managing both AFib and CHF.
A heart-healthy diet rich in fruits, vegetables, whole grains, lean proteins, and healthy fats supports cardiovascular function. Limiting sodium intake is particularly important for patients with heart failure because it helps reduce fluid retention.
Regular physical activity improves cardiovascular fitness, blood pressure control, and weight management. Patients should work with their healthcare providers to develop safe exercise programs appropriate for their condition.
Smoking cessation is essential because tobacco use damages blood vessels, increases cardiovascular risk, and worsens overall heart health.
Alcohol intake should be limited, especially in patients with AFib, as excessive alcohol consumption can trigger arrhythmias.
Stress management techniques such as meditation, yoga, deep breathing exercises, and counseling may also support overall cardiovascular wellness.
When to Seek Immediate Medical Attention
Certain symptoms require prompt evaluation.
Sudden chest pain, severe shortness of breath, fainting, rapid swelling, confusion, or signs of stroke such as facial drooping, weakness, or difficulty speaking should be treated as medical emergencies.
Patients experiencing new or worsening palpitations, unexplained weight gain, or significant changes in symptoms should contact their healthcare provider as soon as possible.
Conclusion
Atrial fibrillation and congestive heart failure are distinct cardiovascular conditions, yet they frequently coexist and influence one another. AFib is primarily an electrical disorder characterized by an irregular heartbeat, whereas CHF is a mechanical disorder involving impaired pumping function and fluid accumulation.
Despite their differences, both conditions can significantly impact quality of life and increase the risk of serious complications. Understanding how these diseases develop, recognizing their symptoms, and seeking timely medical care are essential steps toward better outcomes.
Through early diagnosis, appropriate treatment, healthy lifestyle choices, and close collaboration with healthcare providers, many individuals with AFib, CHF, or both conditions can successfully manage their symptoms and maintain active, fulfilling lives. Knowledge, vigilance, and proactive care remain some of the most powerful tools for protecting long-term heart health.
Disclaimer
This article is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment. Seizures, severe headache, confusion, visual changes, or blood pressure readings in the hypertensive crisis range require urgent medical evaluation.