

Sleep Apnea & Pulmonary Hypertension: Understanding the Link Between Two Silent Threats
Introduction
Sleep apnea and pulmonary hypertension (PH) each pose serious health risks on their own, but when they coexist, the consequences can be even more significant. In this post, we’ll explore how obstructive sleep apnea (OSA) can lead to or worsen, pulmonary hypertension, why early recognition matters, and what you can do to protect your heart and lungs. Whether you’re a patient, caregiver, or healthcare professional, this guide will help you understand the science, spot warning signs, and pursue effective treatment.

1. Defining the Players
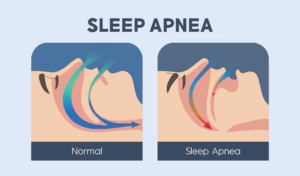
1.1 What Is Obstructive Sleep Apnea (OSA)?
• A sleep disorder characterized by repeated upper-airway collapse during sleep
• Leads to intermittent oxygen desaturations, sleep fragmentation, and daytime fatigue
• Risk factors: obesity, neck circumference >17″, male gender, family history
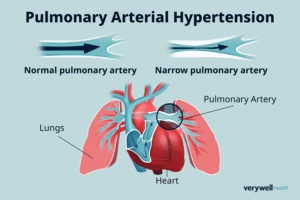
1.2 What Is Pulmonary Hypertension?
• Elevated blood pressure in the pulmonary arteries (≥25 mm Hg at rest)
• Stresses the right ventricle, can lead to right-sided heart failure (cor pulmonale)
• Classified into five groups by cause: pulmonary arterial hypertension, left-heart disease, lung disease/hypoxia (including OSA), chronic thromboembolism, and unclear mechanisms
2. How OSA Drives Pulmonary Hypertension
2.1 Intermittent Hypoxia & Vascular Remodeling
• Repeated drops in blood oxygen trigger vasoconstriction in lung vessels
• Over time, this promotes smooth-muscle proliferation and stiffening of pulmonary arteries
2.2 Sympathetic Nervous System Activation
• Arousal from apneas spikes heart rate and blood pressure
• Chronic sympathetic overdrive contributes to systemic and pulmonary hypertension
2.3 Inflammation & Endothelial Dysfunction
• OSA-related oxidative stress inflames blood vessels
• Damaged endothelium loses its ability to dilate properly, boosting vascular resistance
3. Recognizing the Signs
3.1 Symptoms to Watch For
• Loud snoring, witnessed apneas, gasping or choking during sleep
• Excessive daytime sleepiness, morning headaches, difficulty concentrating
• Shortness of breath on exertion, chest discomfort, leg swelling
3.2 When to Screen for PH in OSA Patients
Consider referral for echocardiography or right-heart catheterization if you see:
• Unexplained dyspnea despite good CPAP adherence
• Signs of right-ventricular strain on ECG or imaging
• Elevated NT-proBNP or other markers of cardiac stress
4. Diagnosis & Testing
4.1 Sleep Studies (Polysomnography)
• Records airflow, blood oxygen levels, brain waves, and muscle activity
• Defines apnea-hypopnea index (AHI): the number of breathing interruptions per hour
4.2 Cardiac & Pulmonary Evaluation
• Transthoracic echocardiogram estimates pulmonary artery pressure and RV function
• Right-heart catheterization remains the gold standard for confirming PH
• Pulmonary function tests and overnight oximetry assess baseline lung health
5. Treatment Strategies
5.1 Continuous Positive Airway Pressure (CPAP)
• First-line therapy for OSA, splints open the airway, prevents apneas
• Improves oxygenation, reduces sympathetic tone, may lower pulmonary pressures
5.2 Supplemental Oxygen & Lifestyle Changes
• Nocturnal oxygen can blunt hypoxic vasoconstriction in some patients
• Weight loss, exercise, and alcohol avoidance enhance OSA control
5.3 Pulmonary Hypertension–Targeted Therapies
• Endothelin receptor antagonists, phosphodiesterase-5 inhibitors, prostacyclin analogs
• Reserved for patients with persistent PH despite optimized OSA treatment
6. Prevention & Long-Term Management
• Early identification of snoring and daytime sleepiness, don’t ignore the signs
• Regular follow-up with sleep specialists and cardiologists
• Emphasize adherence to CPAP, smoking cessation, and heart-healthy diet
• Monitor weight, blood pressure, and symptoms every 6–12 months
Conclusion
Sleep apnea and pulmonary hypertension form a vicious cycle: untreated OSA fuels vascular changes that raise pulmonary pressures, while PH symptoms can mask or delay OSA diagnosis. The good news is that timely recognition and comprehensive treatment, starting with CPAP therapy and stretching into targeted PH medications when needed, can break this cycle. If you or a loved one snores loudly, wakes gasping for air, or struggles with unexplained breathlessness, don’t wait. Talk to your healthcare provider about a sleep study and cardiac evaluation. By intervening early, you’ll protect your heart, improve your quality of life, and breathe easier, night and day.








One Response