Portal Hypertension ICD-10: A Comprehensive Guide to Accurate Coding
Portal hypertension is a clinically significant condition frequently encountered in gastroenterology and hepatology. From a health systems perspective, accurate ICD-10 coding of portal hypertension is essential not only for reimbursement, but also for clinical documentation integrity, epidemiological surveillance, and coordinated patient care.
- Use correct ICD-10 codes: K76.6 for portal hypertension; I85.00/I85.01 for varices; R18.0 ascites; D73.5 splenomegaly.
- Document etiology, presence and severity of complications, relevant imaging and labs, and procedures performed to support accurate coding.
- Follow stepwise coding: assign primary code, add separate complication codes, code associated conditions, sequence by clinical priority, ensure specificity.
- Avoid common pitfalls: omit complications, incorrect sequencing, incomplete documentation, and overreliance on encoders; perform audits and educate providers.
Coding errors, particularly omissions of complications or incorrect sequencing, may lead to claim denials, underpayment, or misrepresentation of disease severity. Therefore, a clear understanding of the clinical basis of portal hypertension, the appropriate ICD-10 codes, and the documentation requirements is necessary for coders, billers, and healthcare providers.
This guide provides a detailed and structured explanation of:
- The pathophysiology of portal hypertension
- The correct ICD-10 code and related codes
- Documentation requirements for accurate coding
- Step by step coding guidelines
- Common pitfalls and compliance strategies
What Is Portal Hypertension?
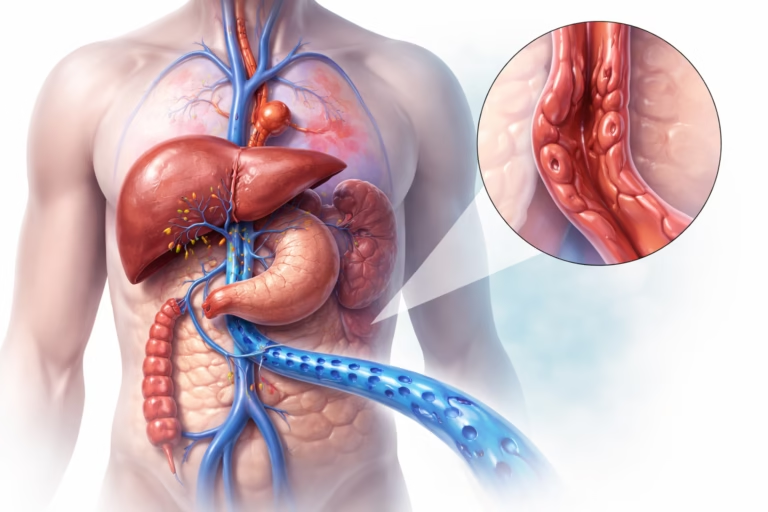
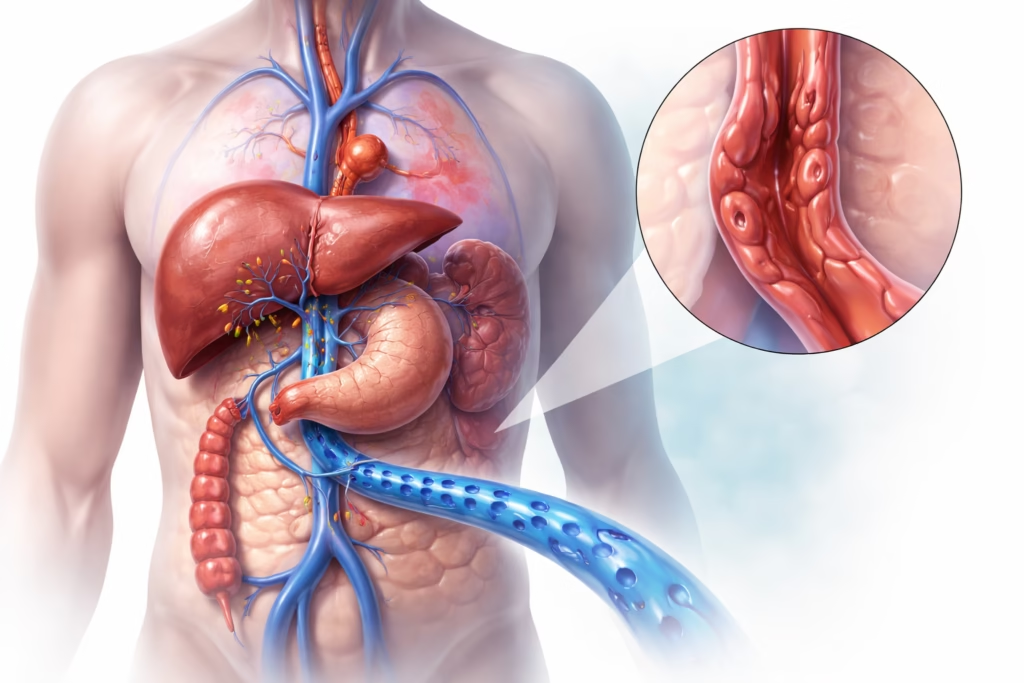
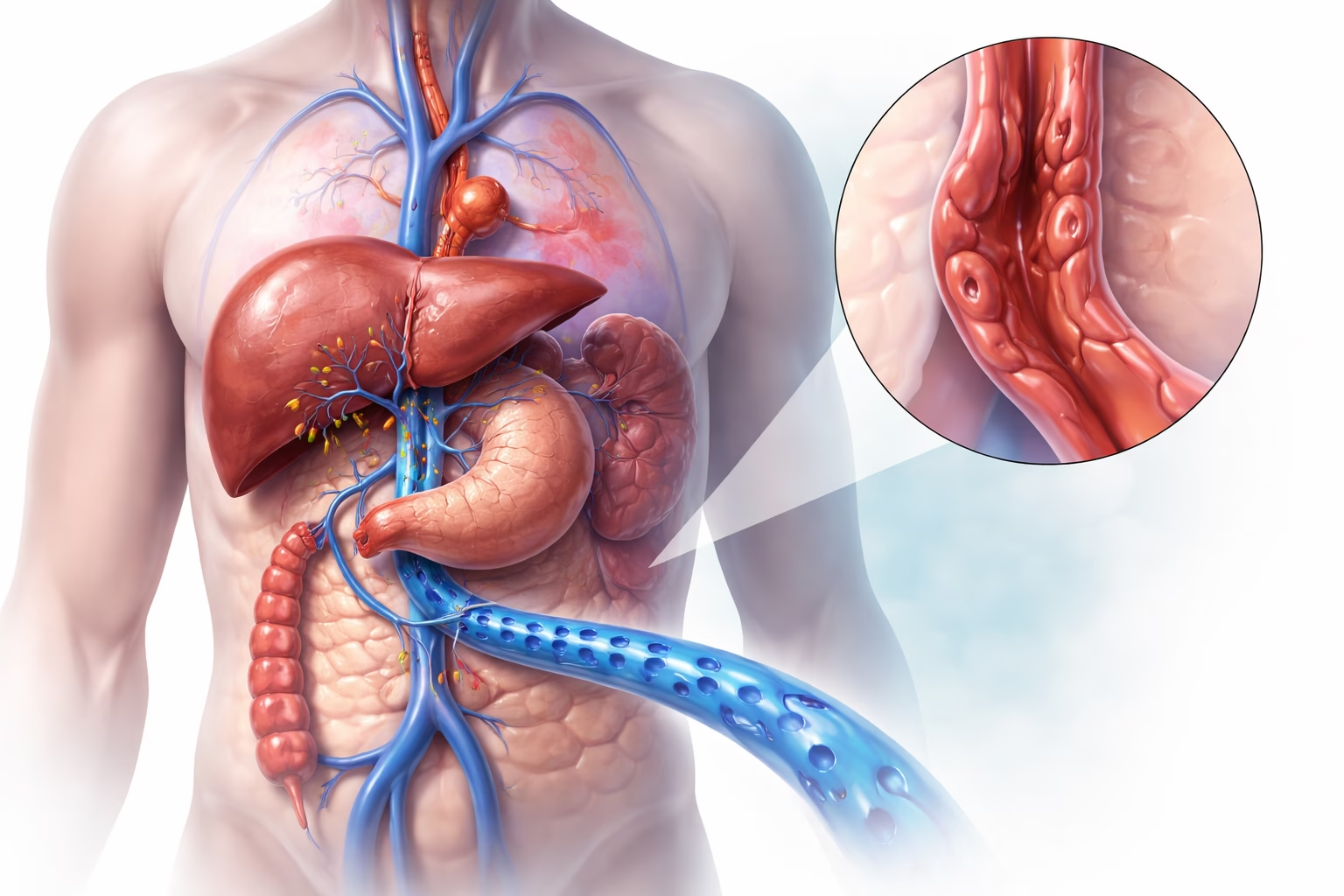
Portal hypertension refers to elevated blood pressure within the portal venous system, which is the vascular network responsible for transporting blood from the gastrointestinal tract, spleen, and pancreas to the liver.
Pathophysiology Explained
Under normal conditions, blood flows through the portal vein into the liver with relatively low resistance. However, when liver architecture is disrupted, most commonly due to cirrhosis, resistance to blood flow increases. As a result, pressure builds up in the portal system.
This increased pressure leads to several physiological changes:
- Increased resistance to portal blood flow: Scar tissue in cirrhosis compresses blood vessels, restricting normal circulation
- Development of collateral circulation: The body forms alternative pathways for blood flow, including esophageal and gastric varices
- Backflow effects on organs: The spleen enlarges due to congestion, and fluid may accumulate in the abdomen
Common Causes
- Liver cirrhosis (most common cause)
- Portal vein thrombosis
- Schistosomiasis (in endemic regions)
- Chronic liver diseases such as nonalcoholic steatohepatitis
Clinical Manifestations
Symptoms and signs vary depending on severity. Some patients may initially be asymptomatic, while others present with serious complications:
- Ascites: Accumulation of fluid in the abdominal cavity
- Splenomegaly: Enlargement of the spleen due to increased pressure
- Esophageal varices: Dilated veins that may rupture and cause life threatening bleeding
- Hepatic encephalopathy: Altered mental status due to liver dysfunction
Understanding these clinical features is important because ICD-10 coding must reflect not only the primary condition but also its complications.
ICD-10 Classification for Portal Hypertension
The ICD-10 system provides standardized codes used globally for disease classification and billing.
Primary Code
- K76.6 – Portal hypertension
This code is used when portal hypertension is diagnosed and documented. It represents the underlying condition but does not capture complications, which must be coded separately.
Related Codes for Common Complications
Portal hypertension is rarely an isolated condition. Therefore, additional codes are often required to fully represent the clinical scenario.
- I85.00 – Esophageal varices without bleeding
Used when varices are present but have not ruptured - I85.01 – Esophageal varices with bleeding
Used when there is active or recent bleeding, which is a serious complication - R18.0 – Ascites
Used when fluid accumulation in the abdomen is documented - D73.5 – Splenomegaly, not elsewhere classified
Used when spleen enlargement is identified
These additional codes are essential because they reflect disease severity and influence reimbursement and care planning.
Documentation Essentials
Accurate ICD-10 coding depends heavily on the quality and completeness of clinical documentation. Without detailed documentation, even experienced coders may be unable to assign the correct codes.
Etiology
The underlying cause of portal hypertension should be clearly stated. For example:
- Cirrhosis (alcohol related or nonalcoholic)
- Portal vein thrombosis
- Infectious or parasitic causes
This helps ensure that both the primary disease and its complications are properly captured.
Severity and Complications
Documentation should specify whether complications are present and their severity. For instance:
- Presence or absence of variceal bleeding
- Degree of ascites (mild, moderate, refractory)
- Evidence of hepatic encephalopathy
This level of detail allows coders to assign additional codes accurately.
Associated Findings
Other clinical findings such as splenomegaly, thrombocytopenia, or abnormal imaging results should be documented. These findings provide supporting evidence for the diagnosis and may influence coding decisions.
Procedures and Interventions
Procedures performed to manage portal hypertension should also be recorded, including:
- Transjugular intrahepatic portosystemic shunt (TIPS) placement
- Endoscopic variceal band ligation
- Paracentesis for ascites
These details are important for both procedural coding and overall clinical context.
Documentation Checklist
To ensure completeness:
- Confirm that “portal hypertension” is explicitly stated
- Document all complications clearly
- Include relevant imaging and laboratory findings
- Record treatments and outcomes
Incomplete documentation is one of the most common reasons for coding errors and claim denials.
Step by Step Coding Guidelines
Accurate coding follows a structured process. Each step ensures that all aspects of the patient’s condition are captured.
Step 1: Identify the Primary Diagnosis
If portal hypertension is documented without complications, assign:
- K76.6 – Portal hypertension
This serves as the base code.
Step 2: Capture Complications Separately
If complications such as varices or ascites are present, they must be coded in addition to the primary diagnosis.
For example:
- Use I85.01 if there is variceal bleeding
- Use I85.00 if varices are present without bleeding
This step is crucial because complications often drive clinical severity and reimbursement levels.
Step 3: Code Related Conditions
Additional associated conditions should also be coded when documented:
- R18.0 for ascites
- D73.5 for splenomegaly
This ensures a complete clinical picture.
Step 4: Sequence Codes Correctly
Code sequencing reflects clinical priority. The most serious or resource intensive condition is listed first.
For example:
- If variceal bleeding is present, I85.01 should be listed before K76.6
- If no bleeding is present, K76.6 may remain the primary code
Correct sequencing is essential for proper claim processing.
Step 5: Ensure Specificity
ICD-10 coding emphasizes specificity. Coders should avoid vague or incomplete coding when more detailed information is available.
Although portal hypertension itself does not involve laterality, complications and related diagnoses should be coded as precisely as possible.
Common Pitfalls and How to Avoid Them
Omission of Complications
One of the most frequent errors is failing to code complications such as variceal bleeding. This leads to underrepresentation of disease severity and potential underpayment.
Incorrect Sequencing
Listing portal hypertension as the primary diagnosis when a more severe complication is present may result in coding inaccuracies.
Incomplete Documentation
If providers do not clearly document the condition and its complications, coders may be unable to assign the correct codes. This highlights the importance of provider education.
Overreliance on Encoder Software
While coding software can assist, it should not replace clinical judgment. Coders should always verify suggested codes against documentation.
Clinical Coding Examples Explained
Example 1
A 58 year old patient with alcoholic cirrhosis presents with melena. Endoscopy confirms bleeding esophageal varices.
Coding:
- I85.01 – Esophageal varices with bleeding
- K76.6 – Portal hypertension
- K70.30 – Alcoholic cirrhosis of liver without ascites
In this case, variceal bleeding is the most critical condition and is therefore listed first.
Example 2
A 65 year old patient with nonalcoholic steatohepatitis develops ascites and splenomegaly without bleeding.
Coding:
- K76.6 – Portal hypertension
- R18.0 – Ascites
- D73.5 – Splenomegaly
- K75.81 – Nonalcoholic steatohepatitis
Here, portal hypertension is the primary diagnosis, with associated complications coded separately.
Tips for Compliance and Quality Assurance
Conduct Regular Audits
Periodic review of coded cases helps identify patterns of errors and ensures adherence to guidelines.
Educate Healthcare Providers
Providers should understand the importance of documenting details such as “with bleeding” or “without bleeding,” as this directly affects coding accuracy.
Use Coding Tools Carefully
Encoder software should be used as a support tool, not as a substitute for proper review.
Stay Updated
ICD-10 guidelines are updated regularly. Coders should consult official resources such as CMS and WHO to remain current.
Conclusion
Accurate coding of portal hypertension using ICD-10 code K76.6 requires more than simply identifying the diagnosis. It involves a detailed understanding of the condition, recognition of associated complications, careful documentation, and proper sequencing of codes.
By applying structured coding practices, healthcare professionals can improve reimbursement accuracy, reduce claim denials, and ensure that patient records accurately reflect clinical complexity. Ultimately, precise coding contributes to better healthcare data, improved patient management, and stronger health system performance.
Call to Action
To remain informed about evolving ICD-10 standards, best practices, and updates in medical coding, consider subscribing to trusted healthcare education resources and professional updates. Staying current is essential for maintaining coding accuracy and compliance.